50 YEAR OLD FEMALE WITH CKD AND DENOVO HTN
This is a online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patients problems through series of inputs from available global community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs .This E log book also reflects my patient centered online learning portfolio and your valuable inputs in comment box is welcome.
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis” to develop my competency in reading and comprehending clinical data including history , clinical findings , investigations and come up with diagnosis and treatment plan .
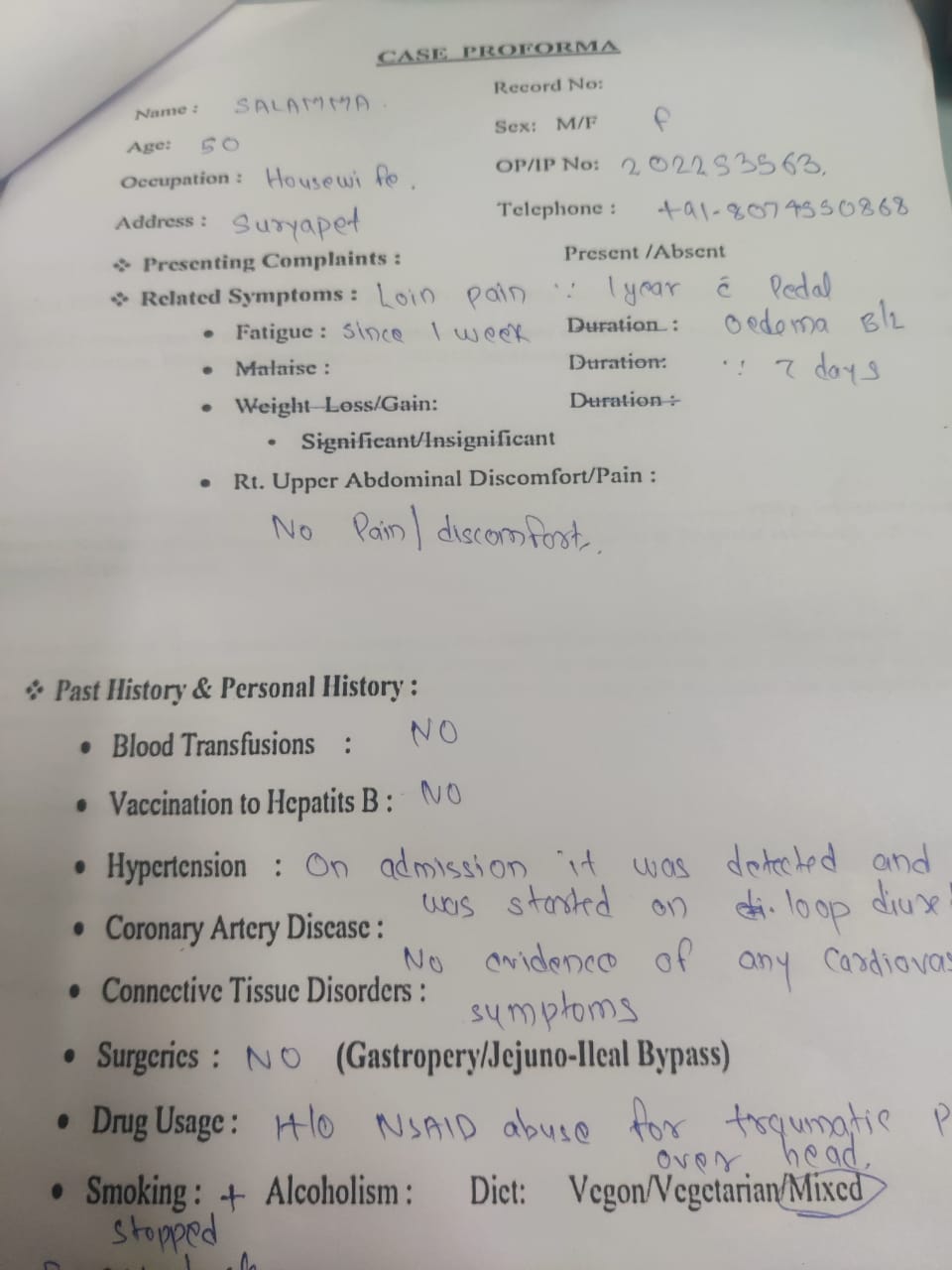
A 50 year old female who is a housewife residing at suryapet Came to casualty with chief complaints of:
Loin pain since 1 year
Pedal edema since 7 days
HOPI :

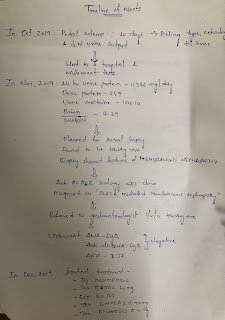
Patient was apparently asymptomatic 5 years back , then she had a fall and sustained head injury (clot in brain according to pt and pt attenders) with severe headache for which she underwent surgery .
Patient complains of loin pain since 3 years which is Insidious in onset , gradually progressive , dragging type , radiating to lower abdomen, intermittent which aggrevated on working and relieved on taking medications ( NSAIDs - been using it since 2 years )
Patient has history of burning micturition since 3 months not associated with pain in lower abdomen, haematuria , vomitings.
Fever on and off since 3 months which is of low grade , intermittent , not associated with chills and rigor with no diurnal variations
Patient has pedal edema since 7 days , pitting type extending till knee joint
No H/O shortness of breath , orthopnea , PND.
Daily routine - She was a daily wage worker , but stopped working from 5 years after sustaining head injury .Stays at home since 5 years , does household works.
Past history:
Denovo HTN
Not a k/c/o DM , epilepsy, asthma, CAD
Personal history:
Appetite - decreased since 3 months
Diet - Mixed
Bladder - burning micturition since 3 months
Bowel habits - regular
Sleep - decreased since 3 months
Family history:
No similar complaints in the family
General examination:
Patient is conscious, coherent, cooperative, well oriented to time , place and person
Pallor - Present

Icterus - absent
Cyanosis - absent
Clubbing - absent
Lymphadenopathy- absent
Pedal edema - pitting type extending till knee


VITALS : Temp - 98.6 F
PR - 82 bpm
BP - 160/80 mmhg
RR - 16 cpm
SPO2 - 98% onRA
GRBS - 119 mg/dl
Systemic examination:
PER ABDOMEN:
Inspection :
Abdomen is obese.


Umbilicus is central and inverted
All quadrants are moving equally with respiration
No scars , sinuses , engorged veins, visible pulsations .
Hernial orifices are free.
Palpitation :
Abdomen is soft and non tender
No organomegaly.
Percussion :
Tympanic note heard over the abdomen.
Auscultation:
Bowel sounds are heard.
CARDIOVASCULAR SYSTEM:
Inspection:
Shape of chest is elliptical.
No raised JVP
No visible pulsations, scars , sinuses , engorged veins.
Palpitation:
Apex beat - felt at left 5th intercostal space
No thrills and parasternal heaves
Auscultation :
S1 and S2 heard.
RESPIRATORY SYSTEM:
Inspection:
Shape- elliptical
B/L symmetrical ,
Both sides moving equally with respiration .
No scars, sinuses, engorged veins, pulsations
Palpation:
Trachea - central
Expansion of chest is symmetrical.
Vocal fremitus - normal
Percussion: resonant bilaterally
Auscultation:
bilateral air entry present. Normal vesicular breath sounds heard.
CENTRAL NERVOUS SYSTEM:
Conscious,coherent and cooperative
Speech- normal
No signs of meningeal irritation.
Cranial nerves- intact
Sensory system- normal
Motor system:
Tone- normal
Power- bilaterally 5/5
Reflexes Right Left
Biceps ++ ++
Triceps ++ ++
Supinator ++ ++
Knee ++ ++
Ankle ++ ++
PROVISIONAL DIAGNOSIS :
CKD secondary to NSAID abuse with denovo HTN.
Investigations :
Hb – 8.2 gm/dl
TLC – 7700cells/cu mm
Neutrophils : 56
Lymohocytes : 29
Eosinophils : 07
Monocytes : 08
Platelets – 2.30 lakh/cu mm
Serum albumin - 3.9 gm/dl on 22/12/22
Serum iron - 50 ug/dl
CUE :
Albumin - ++++
Pus cells - 2-3/HPF
Epithelial cells - 2-3/HPF
Lipid profile :
Total cholesterol - 182
LDL - 108
HDL-48
TG -147
FBS :76 mg/dl
RENAL FUNCTION TESTS :
Urea : 148 mg/dl
Creatinine : 7.5 mg/dl
Sodium : 137 mEq/L
Potassium : 5.7 mEq/L
Chloride : 107 mEq/L
LIVER FUNCTION TESTS :
Total bilirubin : 0.84 mg/dl
Direct bilirubin : 0.19 mg/dl
AST : 10 IU/L
ALT : 10 IU/L
Alkaline phosphate :395 IU/L
Total proteins : 5.6 gm/dl
Albumin : 3.63 gm/dl
A/G ratio : 1.84
CHEST X RAY:

ECG :

USG:

2D echo :

Treatment:
Salt restriction < 2 gm / day
Fluid restriction < 1.5 lit / day
Inj LASIX 40 mg IV BD
T. NICARDIA 10mg PO/TID
T. SHELLCAL 500 mg PO/OD
T.BIO D3 PO/OD
T.NODOSIS 500 mg PO/ BD
T. MET XL 50 mg PO/OD
FINAL DIAGNOSIS:
CKD secondary to NSAID abuse with denovo HTN with grade 1 fatty liver.






Comments
Post a Comment